


 Sign Out
Sign Out
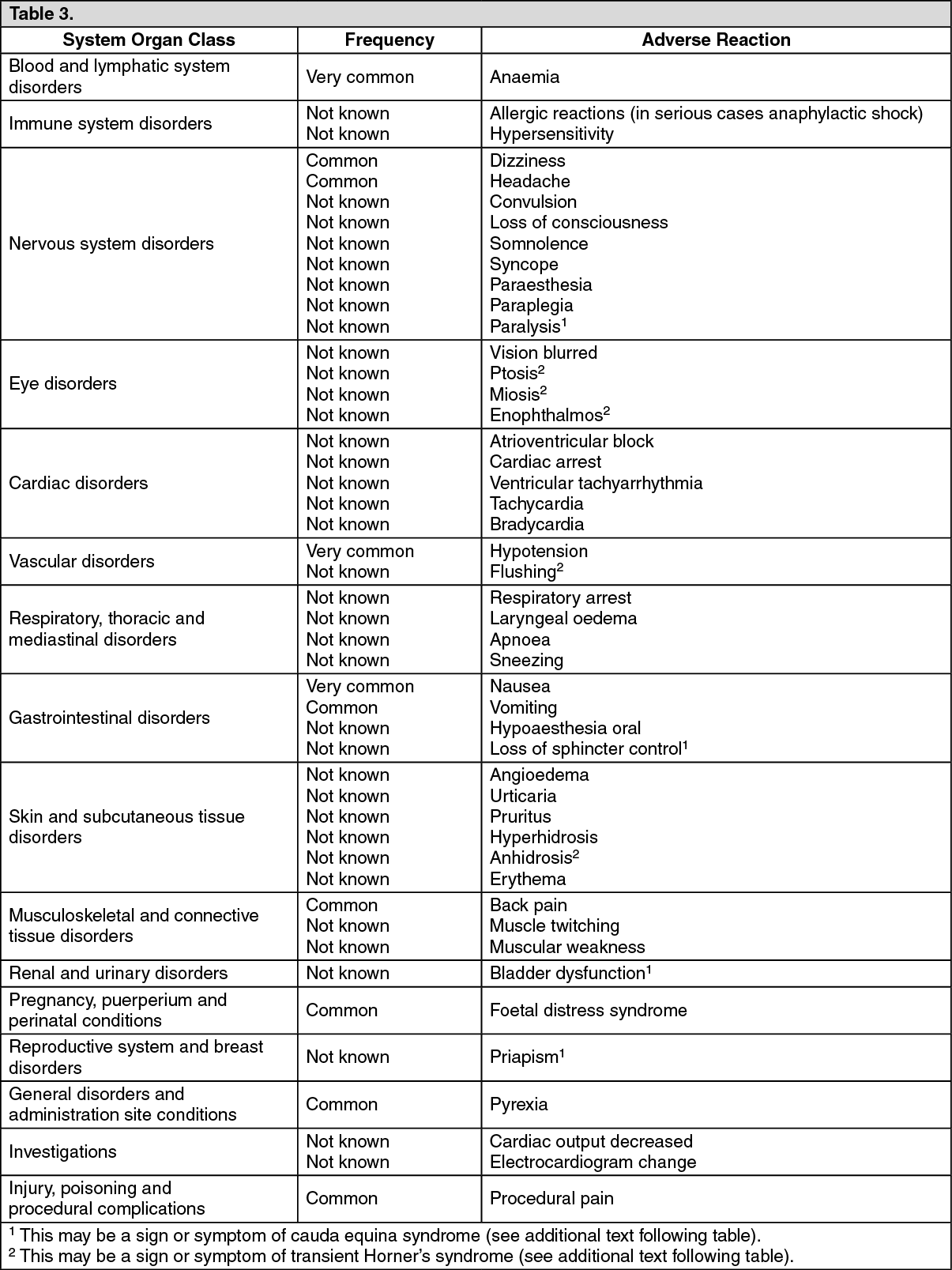
Adverse reactions reported either spontaneously or observed in clinical trials are depicted in the following table. Within each system organ class, the adverse drug reactions are ranked under headings of frequency, using the following convention: Very common (≥1/10); Common (≥1/100 to <1/10); Uncommon (≥1/1,000 to <1/100); Rare (≥1/10,000 to <1/1,000); Not known (cannot be estimated from the available data). (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdverse reactions with local anaesthetics of the amide type are rare, but they may occur as a result of overdosage or unintentional intravascular injection and may be serious.
Cross-sensitivity among members of the amide-type local anesthetic group have been reported (see Contraindications).
Accidental intrathecal injection of local anaesthetics can lead to very high spinal anaesthesia.
Cardiovascular effects are related to depression of the conduction system of the heart and a reduction in myocardial excitability and contractility. Usually these will be preceded by major CNS toxicity, i.e. convulsions, but in rare cases, cardiac arrest may occur without prodromal CNS effects.
Neurological damage is a rare but well recognised consequence of regional and particularly epidural and spinal anaesthesia. It may be due to direct injury to the spinal cord or spinal nerves, anterior spinal artery syndrome, injection of an irritant substance or an injection of a non-sterile solution. Rarely, these may be permanent.
There have been reports of prolonged weakness or sensory disturbance, some of which may have been permanent, in association with levobupivacaine therapy. It is difficult to determine whether the long-term effects were the result of medication toxicity or unrecognized trauma during surgery or other mechanical factors, such as catheter insertion and manipulation.
Reports have been received of cauda equina syndrome or signs and symptoms of potential injury to the base of the spinal cord or spinal nerve roots (including lower extremity paraesthesia, weakness or paralysis, loss of bowel control and/or bladder control and priapism) associated with levobupivacaine administration. These events were more severe and in some cases did not resolve when levobupivacaine was administered for more than 24 hours (see Precautions).
However, it cannot be determined whether these events are due to an effect of levobupivacaine, mechanical trauma to the spinal cord or spinal nerve roots, or blood collection at the base of the spine.
There have also been reports of transient Horner's syndrome (ptosis, miosis, enophthalmos, unilateral sweating and/or flushing) in association with use of regional anaesthetics, including levobupivacaine. This event resolves with discontinuation of therapy.
View ADR Monitoring Form